
An ancient fungus lurks in Southwestern soils. A saguaro grows on a hillside near Superstition Mountain, Arizona. Tom Driggers via Flickr
Jessica Cooley, a 33-year-old educator in New Jersey, had never gardened before. This June, as a camp counselor, she first used organic potting soil, packaged in California and purchased locally. A week later, Cooley, who suffers from asthma, developed a cough. It wouldn’t go away. After three and a half weeks, she visited the hospital but was discharged because her chest X-ray showed no pulmonary abnormalities.
Jessica Cooley, a 33-year-old educator in New Jersey, used organic potting soil, packaged in California and purchased locally. A week later, Cooley, who suffers from asthma, developed a cough.
Her own research found that her symptoms, including persistent cough and chest pain, aligned closely with those of Valley fever, a fungal infection endemic to Arizona and California whose spores target the lungs. Since she hadn’t visited the Southwest, the only source she could think of was the potting soil.
Her New Jersey physicians remained unconvinced, until a blood test confirmed she had the fungal infection caused by airborne inhalation of the spores of the Coccidioides fungus, which thrives within the soil and dust of dry, arid environments in the Southwest and regions of Mexico, Central, and South America.
Cooley’s case is a sign that Valley fever is now spreading farther and farther from the regions where it originally flourished. It comes at a time of a sharp rise in reported cases in its endemic regions. According to the states’ public health departments, California’s caseload rose from 4,419 in the year ending August 31, 2023 to 7,613 in 2025 and Arizona’s rose from 10,990 in 2023 to 14,640 in 2024.

Cooley’s struggle with the disease is a reminder of both its increasing prevalence, its persistence and the medical community’s spotty understanding of it. After several doctor visits, Cooley realized that few physicians in the Northeast were familiar with Valley fever, let alone knew how to treat it. Her doctors’ remedy, a prednisone prescription, suppressed her immune system, allowing the fungus to grow. “Just because a disease is localized to one region doesn’t mean people in other regions shouldn’t be knowledgeable about it,” Cooley said. “It’s just not on anyone’s radar in this area.”
Cooley is well on her way to recovery. But Julie Russell, who contracted Valley fever in 2018 as a Florida resident after staying in the camper of a friend who had visited Arizona, has yet to recover. “It’s really, really frustrating to deal with the doctor when they try to tell you things that are not true, to get to feel like you’re getting the care that you really need,” said Russell, who relocated to her rural home in Indiana to be closer to family as she continues to battle the disease.
An uptick in Valley fever cases

A little-remarked fixture of the Southwest for decades, Valley fever is now infecting new populations – like those attending a Kern County music festival. The data for California and Arizona show the highest annual increase on record for both states; the most recent figures from the CDC show 21,171 cases nationally in 2023, the second-highest in the last quarter-century. A CDC report also shows that from 1999 through 2023, an average of 200 people annually died from Valley fever.

John Galgiani, a University of Arizona professor and director of the Valley Fever Center for Excellence in Tucson who has studied the disease for four decades, noted that virtually anyone can contract the disease. “If you inhale a spore of the fungus… after an incubation period of one to three weeks, those people who get sick will often have respiratory symptoms. It can be thought to be a community acquired pneumonia, mistakenly thought to be bacterial or viral.”
“If you inhale a spore of the fungus … after an incubation period of one to three weeks, those people who get sick will often have respiratory symptoms.”
John Galgiani, Valley Fever Center for Excellence, University of Arizona
More than a century after Valley fever was first identified in the San Joaquin Valley, and three decades after a severe outbreak in Kern County established it as a nationally reportable disease, treatment remains challenging for many patients.
While a range of antifungal treatments are available, these can have side effects, including gastric issues, rashes, and even organ damage. Researchers at the University of Arizona in Tucson are working on a vaccine targeting Valley fever in dogs, and hope to use this model to develop a vaccine for humans.
Scientists attribute the rise in Valley fever cases in the Southwest — with a 73 percent increase in Arizona and quadrupling of cases in California over the past decade — to both climate change and population growth: the region is a warming hotspot and home to some of the nation’s fastest-growing areas. While the national numbers fluctuate, there has also been a quadrupling of national cases between 2001 and 2022, from fewer than 5,000 to more than 20,000.
As climate change leads to higher temperatures and drier environments — ideal conditions for the spread of the spores of the Coccidioides fungus — the disease has increasingly spread around the West, as far north as Washington, Oregon, Idaho, and Montana and as far east as west Texas, the Dakotas and Nebraska. Patients like Russell in Florida and Cooley in New Jersey show that the disease can infect people far beyond the endemic region.
A disease that settles in the lungs but can spread much farther, often while evading diagnosis
Sixty percent of diagnosed patients are asymptomatic or experience mild flu-like symptoms. However, a small percentage suffer symptoms such as cough, chest pain and fatigue associated with a severe form of the disease known as disseminated Valley fever. When the fungus spreads beyond the lungs, it can infect the skin, bones, joints and brain.
Individuals with chronic or disseminated disease require aggressive medical treatment including antifungal medications – sometimes for a lifetime – and potentially surgical intervention.
Many of these patients develop chronic lung disease like Russell, or skin infections and meningitis. Unlike the vast majority of patients with mild Valley fever, individuals with chronic or disseminated disease require aggressive medical treatment including antifungal medications – sometimes for a lifetime – and potentially surgical intervention.
In endemic areas, the fungus causes 10 to 30 percent of “community acquired” pneumonia. Valley fever is estimated to infect more than 200,000 people in the U.S. annually, according to the CDC. This estimate takes into account the many asymptomatic cases and a massive number of underdiagnoses, owing to lack of widespread public awareness.
“It’s really a huge priority for us to raise awareness, not just among Californians, but [non-residents], because this is a disease that may start impacting more and more people throughout the nation,” said Gail Cooksey, a California Department of Public Health (CDPH) epidemiologist. “This is a disease that isn’t getting enough attention and doesn’t get the attention it deserves,” said Tom Chiller, former Chief of the Mycotic Diseases Branch at the CDC. Even in its home areas, “We still see patients who will be misdiagnosed and given multiple courses of antibiotics before someone thinks to… test for Valley fever.”
A steep and growing economic cost
The cost of disseminated, or long-term, Valley fever can be steep – for individuals, families and the nation as a whole. According to a 2010 cost of illness study, Valley fever complications can cost a patient in California more than $1 million over their lifetime in direct medical costs. The numbers are similar for a patient in Arizona. In some states, disseminated Valley fever does not qualify as a disability that would make the patient eligible to receive workers’ compensation.
Valley fever complications can cost a patient in California more than $1 million over their lifetime in direct medical costs.
For other patients, like Cooley and Russell, misdiagnosis and treatment for the wrong disease cause unnecessary costs. “The costs of Valley fever to our economy, to our people, are very substantial, and it’s a drain on our economy that really needs to be paid attention to, because it’s underrecognized and underreported,” said Thomas Gill, a professor of Earth, Environmental and Resource Sciences at the University of Texas El Paso.
Over the 2000-2015 period, the disease cost the nation roughly $3.9 billion annually, Gill noted, although this cost is likely much higher when accounting for underreported cases. In the worst case scenarios for climate change, researchers estimate that the total yearly cost of Valley fever may double by 2050.
A “western Lyme disease?” The East’s tick-borne illness also has long-term complications, but a higher profile
The limited medical knowledge of Valley fever outside the Southwest is in striking contrast to other well-known endemic illnesses, like Lyme disease. True, Lyme disease, a tick-borne bacterial ailment, now has a much broader distribution than Valley fever, encompassing much of the Northeast, the Mid-Atlantic and upper Midwest. But three decades ago, the geographic reach of Lyme disease was as limited as Valley fever’s is today.
“A lot of people have heard of Lyme disease, whereas you couldn’t say the same for Valley fever.”
Tom Chiller, former Chief of the Mycotic Diseases Branch at the CDC
The difference? “The Lyme disease patient community is very active, and they’ve done a great job of raising awareness and that has caught the attention of many people, and I don’t think we’ve seen anything close to that from the Valley fever community, CDC’s Chiller said, adding, “A lot of people have heard of Lyme disease, whereas you couldn’t say the same for Valley fever,” which tends to more often infect a less affluent population. The potential cognitive and cardiac complications of long-term Lyme disease are far better known than the equally debilitating complications of disseminated Valley fever.
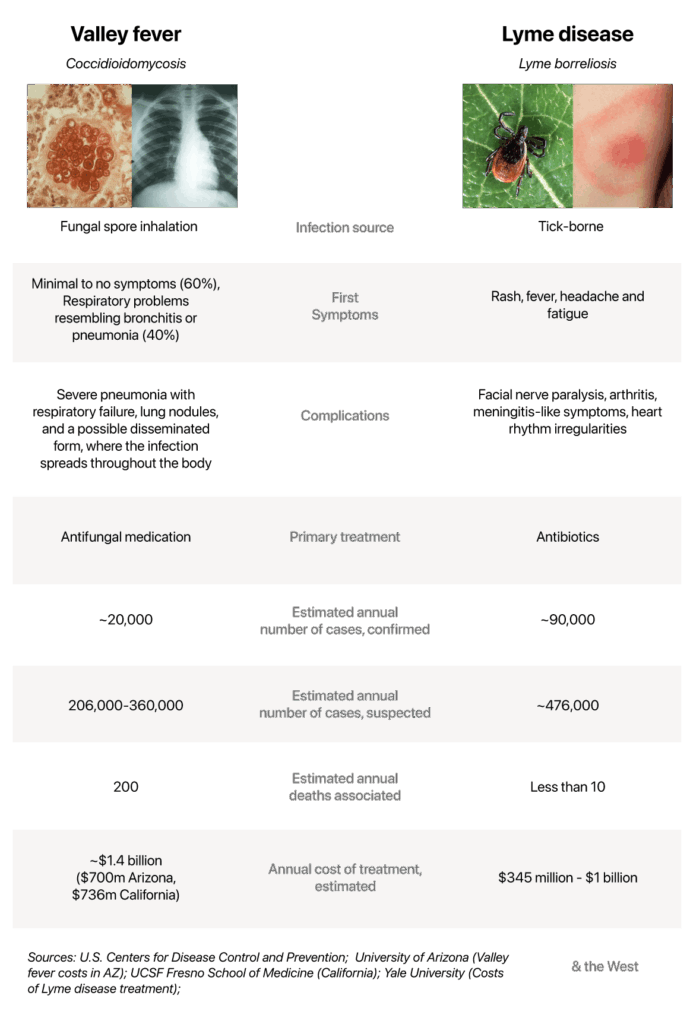
Several high-profile celebrities – most recently Justin Timberlake – have talked about the impact of Lyme disease, which, like Valley fever and COVID-19, has flu-like symptoms including fever, headache, fatigue, and muscle aches. It can also result in death or life-long complications. But decades can pass without news of a well-known Valley fever patient, like the Cincinnati Reds’ catcher, Johnny Bench, who had surgery to remove a lung lesion after playing with Valley fever during his MVP season in 1972.
“They are very regional diseases, but different regions. There’s a lot of interest in academic hospitals in the regions where Lyme is important, so it gets a lot of attention, whereas in the Southwest we’re far the National Institutes of Health and we’re more spread out geographically, so sometimes it feels a little harder to get some momentum around advancing science on this disease,” said Thomas Grys, a researcher at the Mayo Clinic.
Two crises converge: Valley fever and climate change

Other byproducts of climate change, including more frequent and severe dust storms, the explosive growth of wildfires, and an historic megadrought escalate the threat of Coccidioides.
The effects of climate change in the Southwest are easy to observe — more frequent and intense heat waves, droughts, and wildfires. Other changes, such as the spread of Coccidioides spores, may be less visible but are no less impactful. “Fungi are incredible adapters. They are great at finding their niches and spreading and growing and surviving. That’s what they’ve done for tens of millions of years,” Chiller said. “Because of environmental changes, we’re seeing more areas perfectly adapted for these spores to grow.”
Scientists link the rising incidence and geographic spread of Valley fever to heat and temperature fluctuations and changes in precipitation. Other byproducts of climate change, including more frequent and severe dust storms, the explosive growth of wildfires, and an historic megadrought escalate the threat of Coccidioides. In the Central Valley, where water restrictions have led farmers to stop planting, the thousands of acres of fallow farmland are a primary contributor to man-made dust storms.
In Utah, the desiccation of the Great Salt Lake has also led to the spread of dust clouds into urban communities. While further research is necessary to confirm that climate change fuels Valley fever’s increasing spread and severity, scientists see a clear association between a warming climate and higher case counts. “In general, there’s a stronger correlation between dust – including the number of dust storms and the frequency of dust storms – to Valley fever infection than other climate factors … in Arizona,” said Daniel Q. Tong, a professor of Atmospheric, Oceanic and Earth Sciences at Virginia’s George Mason University and co-author of a 2017 study that identified the relationship between dust storms and Valley fever. “We have seen increasing attention to the disease. But is that enough? I don’t think so,” Tong said.

“It’s enigmatic where and how and under what circumstances the spores of the fungus that cause the fever get into the air and when they don’t.”
Thomas Gill, Professor of Earth, Environmental and Resource Sciences at the University of Texas El Paso
According to Tong, the rate of dust storms in the Southwest has risen 10 times faster than the global level over the past several decades, driven by climate change and water diversions. Until the funding was recently cancelled, Tong’s team was engaged in NASA-supported research to uncover the biophysical mechanisms behind the fungus’s spread and to monitor the evolution of dust storms. “It’s enigmatic where and how and under what circumstances the spores of the fungus that cause the fever get into the air and when they don’t. It’s still one of the real known unknowns about the spread of Valley fever,” Gill said.
Recognizing the importance of strengthened public awareness, Gill and Tong call for comprehensive early warning systems – similar to air-quality alerts – so people can reduce their exposure. Tong wants researchers in geology, biology and medicine to collaborate and “tackle this problem from the beginning to the end, establish a cause-effect chain, and use that to inform policymaking and the public.”
Disproportionate impact on the most vulnerable

Outdoor laborers are at the greatest risk – farmworkers, construction workers, and firefighters exposed to disturbed soil. In a 2020 study, Stephen McCurdy and others found that dust exposure is connected to a “near doubling of the odds” of coccidiomycosis. Handling root and bulb vegetables nearly tripled infection rates.
“Clinicians need to know if a farmer comes in and it’s not flu and it’s not COVID-19, and they should have high suspicions for Valley fever. In some cases, it will be fatal if a health care provider doesn’t recognize the disease quickly.”
Elizabeth Strater, the United Farm Workers
The study also identified the impact: 80 percent of the subjects reported fatigue and lost work days. The median of 18.5 lost work days is approximately 10 percent of the average annual workdays of California farmworkers. The study recommended, among other measures, local air and soil sampling during seasons of cultivation, wetting down soil and freshly harvested products, and using high-quality masks.
Elizabeth Strater, a national vice president of the United Farm Workers, a union, thinks health care providers in heavily agricultural areas outside the endemic centers need to be aware of the disease. “Clinicians need to know if a farmer comes in and it’s not flu and it’s not COVID-19, and they should have high suspicions for Valley fever. In some cases, it will be fatal if a health care provider doesn’t recognize the disease quickly.”
Strater believes Valley fever patients merit workers’ compensation. Current protections provided by the state of California for construction workers with respect to Valley fever do not extend to agricultural workers. Reporting they are sick “is a difficult decision for farmworkers… especially right now, where they’re going to be fearful of going to their employer, because they may be worried about retaliation based on their immigration status,” she said. “Immigration status is a pre-existing condition when it comes to farmworkers and Valley fever.”
With recent cuts to Medicaid and limited healthcare for immigrants, the disease can be especially burdensome for farm workers. “Not only is there the disproportionate risk to farm workers, there’s now deep and disproportionate harm, because they’re going to have difficulty accessing the healthcare that they need to save their lives,” Strater said.
Galgiani at Arizona’s Valley Fever Center said anyone in the endemic region is at risk. “It’s possible that socioeconomic factors might actually be the big impact of this disease once someone is infected,” he said. “If they have no ability to take time off from work and see a doctor, that may delay diagnosis and proper care…. If they don’t have health insurance, that also might be a big reason for worse outcomes.”

“Unfortunately, prisons were built in highly endemic areas.”
Tom Chiller
Prison inmates are highly susceptible. In 2015, high incidence rates of the disease in two Central Valley prisons, Avenal State Prison and Pleasant Valley, led inmates to file a largely unsuccessful federal class-action lawsuit. “Unfortunately, prisons were built in highly endemic areas,” Chiller said.
Black, Filipino and Latino individuals are more susceptible to disseminated disease. “Recent research has identified certain genetic patterns that predispose people to disseminated disease, and that’s a relatively new finding,” said David A. Stevens, a professor of medicine at Stanford who studies fungal infections. Other susceptible groups, including the Immunocompromised, those with HIV or cancer and transplant recipients, older patients and pregnant women, are at greatest risk of developing severe complications.Since the inmates’ lawsuit, the California Department of Corrections and Rehabilitation (CDCR) has, with CDC guidance, established prevention protocols, gauging prisoners’ susceptibility and confining high-risk individuals outside endemic areas. According to the Public Policy Information Center, approximately 26 percent of state prison inmates are African American men, 48 percent Latino men, and a significant portion Filipino. “CDCR/CCHCS has a long history of taking precautions with patients who may be at risk for Valley fever,” the department’s communications office said in a statement.
Pursuing improved awareness, quicker diagnoses and a vaccine
Detection methods are improving. Thomas E. Grys, a professor of Laboratory Medicine and Pathology at the Mayo Clinic, is collaborating with Dr. Douglas Lake at Arizona State University to develop a new rapid antibody test that diagnoses Valley fever in 10 minutes compared to today’s test, which takes an average of two weeks.
“This test has the possibility of really advancing testing in urgent care settings and emergency departments…”
Thomas E. Grys, a professor of Laboratory Medicine and Pathology at the Mayo Clinic
The serum-based test is expected to become commercially available by year’s end. It should eliminate the prescriptions for useless antibacterial drugs and improve patient outcomes. “This test has the possibility of really advancing testing in urgent care settings and emergency departments, because we can finally give answers back in a timely fashion that should help identify patients sooner,” Grys said.
Ending widespread ignorance remains a top priority. In Maricopa County, only half of individuals who reported Valley fever were tested for the disease during their first health care visit, making “education for individuals and for health care providers really important,” said Jennifer Collins, the county’s epidemiology supervisor. A separate survey showed improvement: fewer than two percent of pneumonia patients were tested for Valley fever in 2019 and 2020; this year the number is greater than 50 percent.
On the federal level, the CDC aims to raise awareness creating a medical school curriculum and offering continuing medical education credits online for primary-care providers. Medical awareness can reduce the severity of patients’ disease.
“You should have the right to know what could happen,” said Sharon Filip, who survived Valley fever and co-founder of the organization Valley Fever Survivor. “At least if you know what the penalties could be for yourself or a family member. You should have that right to know.”
“I believe everyone should be warned about the existence of this debilitating and sometimes deadly disease which is so easily contracted since everyone needs to breathe,” said Sharon Filip, who was stricken with Valley fever and co-founded Valley Fever Survivor, a patient advocacy organization. “If they decide to visit or move there at least they will be aware of the consequences of their decision if someone comes down with Valley fever.”
“I have to wonder if most people do really recover,” said Russell, the patient who apparently caught the disease from her friend’s camper and is still suffering from it. “I found out here east of the Mississippi River that basically the medical community doesn’t know anything about it, if they’ve even heard of it.”
“I believe everyone should be warned about the existence of this debilitating and sometimes deadly disease which is so easily contracted since everyone needs to breathe,” said Sharon Filip, who was stricken with Valley fever and co-founded Valley Fever Survivor, a patient advocacy organization. “If they decide to visit or move there at least they will be aware of the consequences of their decision if someone comes down with Valley fever.”
While case numbers keep going up, researchers at the Valley Fever Center for Excellence continue to develop a human vaccine, as well as improving early diagnostics, and understanding why it affects different patients in different ways. “It’s been exciting, because there are so many ways to make a difference,” Galgiani said. “There’s so much unknown about this disease, that in any direction you can find things that need answers that haven’t been addressed.”
Edited by Felicity Barringer.