
The doctor is in the air The Reno-based cardiologist Chris Rowan is an avid pilot who performs “circuit riding” bringing care to communities along the Sierra Nevadas. Chris Rowan
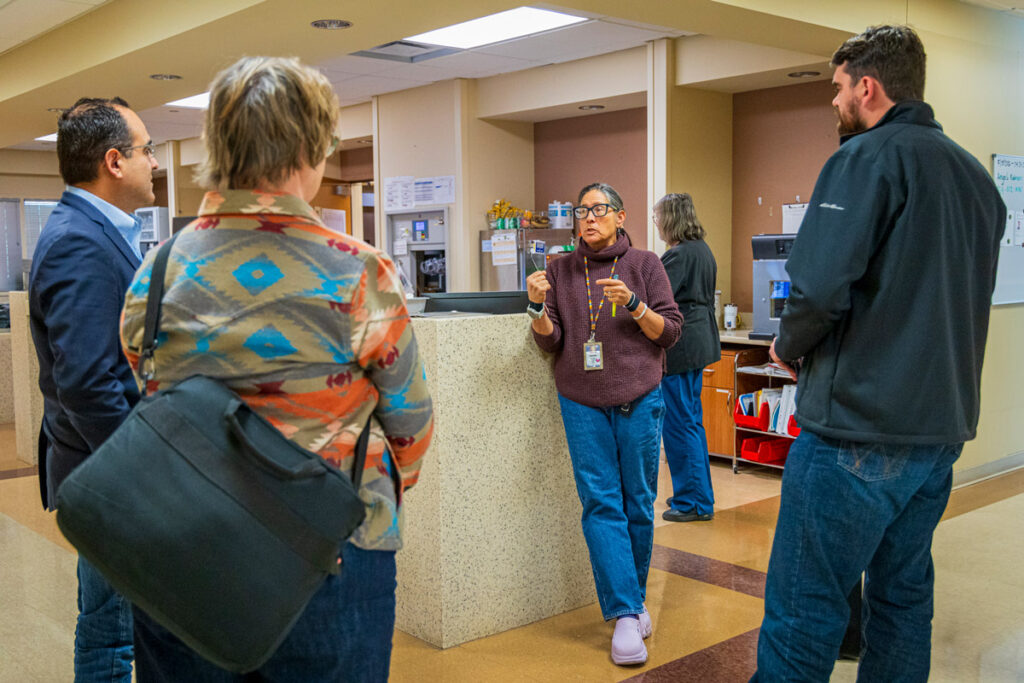
Before 4:15 on Monday mornings, while Nevada is dark, Dr. Chris Rowan gets out of bed, and, via Starbucks, heads to the pilot’s seat on his small four-seat airplane at the Carson City airport. By six, the pilot is wheels-up; by seven, he has touched down 228 miles away in Lone Pine, California, a town of roughly 1,300 tucked beneath Mount Whitney in the Eastern Sierra. He is at Southern Inyo Hospital by eight.
For the next nine hours, Rowan, 52, a cardiologist, and his highly trained nurse, Natalie Thon, see perhaps 50 patients. He’s back home in Reno in time to say goodnight to his three children.


Rowan is a circuit-riding cardiologist, the kind needed to maintain rural cardiac care east of the Sierra. On Tuesday, his destination is Gardnerville, Nevada; on Wednesday, he works in his own office in Reno; on Thursday and Friday, he flies to Bishop, 55 miles north of Lone Pine, sleeping over and flying back Friday evening.
The cardiologist has been a pilot since high school. But for most of his medical career, these vocations never meshed. A few years ago, Rowan left the hospital system in Reno to open his own practice. Then he called rural hospitals within a couple of hundred miles to ask if they needed a cardiologist. Some did.
Rowan will soon extend his circuit to Alturas, a critical access hospital near the Oregon border. When that happens, his seven-day workweek will bring the cardiologist to patients across three states. “It just shrinks your world so much,” he said of his plane. “Now I can serve communities that otherwise just wouldn’t get care.”
An airborne cardiologist tends to a wide-ranging flock
In a given week, Chris Rowan can traverse the Sierra Nevada mountains north to south from his home in Reno, Nevada. Here, the flight tracks from a series of visits from Monday to Friday.
Sources: Chris Rowan; FlightAware.com (flight track data); ESRI (satellite imagery);
Geoff McGhee/& the West
It’s unclear how many specialists are circuit riders like Rowan. Rural hospitals are dotted throughout California, where 95 percent of the landscape is rural but 95 percent of the state population is urban. The hospitals serving rural patients are in increasingly fragile shape, straining to deal with the largest public healthcare cuts in a generation.
For rural communities, healthcare is not just a clinical matter. Its inaccessibility makes it a structural and political issue too.
It’s not just cardiology
Rowan’s trips are an example of how one specialty can be handled in the rural West. What about other services: emergency rooms, anesthesiology, maternity care, cancer treatments, mental health treatment, and medical hardware — machines to do MRIs or EKGs — that make diagnoses possible? As federal funding evaporates, hospitals, to survive, have improvised: merging, sharing specialty coverage, using traveling machines — as five rural hospitals in far northern California do — and, when all else fails, cutting some services to preserve the ones that remain.
Maternity care is often the first to go. One obstetrician can’t handle all the work needed for both normal and complicated deliveries. Obstetric units need neonatologists, anesthesiologists, and nurses. How to pay for all this when not many babies are born there? Many can’t. Dozens of California’s rural hospitals no longer offer labor and delivery at all, leaving expectant mothers to travel towns away from home to give birth.
Medicaid covers nearly half of rural deliveries nationwide; the program faces $1 trillion in cuts over the next decade. Since 2020, four labor and delivery units in California have closed; 34 rural hospitals have no labor and delivery services. In California, the median drive time to hospitals with labor and delivery services is now 49 minutes, Becker’s Hospital Review reported. And things are bad next door: Nevada ranks 46th among all states in OB-GYNs per capita.
Southern Inyo has no obstetrics department. Some women in Lone Pine leave days before their due date to travel to Bishop or Ridgecrest, an hour away. Others wait to go into labor and may deliver in ambulances; others choose to deliver at home.
Dialysis is another frequent casualty: kidney patients, who need treatment three times a week, travel about two and a half times farther in rural areas than urban ones. When a unit closes, a round trip can stretch to 200 miles, KFF Health News reported. When it comes to quality, 40 percent of rural facilities rank at the lowest level in the Centers for Medicare and Medicaid Services’ five-star quality ranking scale, compared to 27 percent of urban centers.
Only the South has sparser dialysis care than the West. Fifty percent of western counties lack any dialysis facility, EBSCO reported.
In emergencies, minutes matter

Often, if hospitals or rural medical facilities choose to stay open, their only remaining service is emergency care. In 2020, federal legislation created the designation “Rural Emergency Hospital Services,” allowing these institutions to collect Medicare benefits.
The stakes of rural geography are easiest to see in emergency care, where distance is its own emergency. In rural communities, emergency departments see 49 percent more patients than their urban counterparts. They serve as the primary — often the only — point of access for a rural population, according to a 2025 study published by the National Library of Medicine.
This strain is seen by the ambulance company first. “We look at 911 as being the front door to healthcare,” said Brian Henricksen, associate vice president for proposal strategy and emergency medical services (EMS) transformation at American Medical Response (AMR), part of Global Medical Response (GMR), the country’s largest provider of ground and air ambulance services.
In communities without urgent care or Federally Qualified Health Center (FQHC) community clinics, residents call 911 because they don’t know another option, he said. So AMR has seen a disproportionate rise in less severe 911 calls — stomach aches, fevers, foot pain, parents unsure how to dose a child’s Tylenol — attributed to “lack of healthcare access, not necessarily a lack of emergency department access.”
When an elderly patient suffered a stroke on U.S. Route 395 in February — the two-lane highway threading through the high-desert Owens Valley east of the Sierra — the nearest hospital was Southern Inyo. For the 150 miles between Lone Pine and Ridgecrest, there was no other hospital. The physicians at Southern Inyo stabilized him, buying valuable time, but could not provide the specialized care he needed.
The nearest stroke center was in Nevada; he was airlifted there. As the patient crossed state lines, so did his medical records, complicating his recovery care with coordination fragmented between Lone Pine, Las Vegas, and Reno. Weeks passed before he got home, months before he got well.
When the last resort closes

“The upside was that we were still here,” said Kevin Flanigan, chief executive of the Southern Inyo Healthcare District. “We could stabilize and expedite his transfer to a stroke center.” The downside was twofold: not only was the patient’s physical care fragmented, his emotional recovery was also compromised by his distance from his family.
Without Southern Inyo, there would be a 150-mile stretch of highway with no emergency care. Stroke victims 150 miles from the next emergency center are “not going to make it,” Flanigan said.
Families can’t afford to stay close. Rowan once airlifted a woman from Bishop to Reno, though her husband begged him not to: the family could not afford the gas for the eight-hour round trip.
Nationwide, 720 rural hospitals — about one in three facilities — are at risk of closure, with 294 facing shutdown in the next two to three years, according to a May 2026 analysis by the Center for Healthcare Quality and Payment Reform.
Many rural facilities are challenged, with a number at risk of closure
Already challenged by small populations and long travel distances, hospitals serving rural patients are in increasingly fragile shape, straining to deal with the largest public healthcare cuts in a generation. A report by the advocacy group Public Citizen identified dozens of rural hospitals in the West that are in danger of closure. A look at rural acute-care hospitals and those designated as at risk, along with the one-hour travel area highlighted around them.
Rural hospitals in the American West
Rural hospitals at risk of closure
Sources: Federal Office of Rural Health Policy (FORHP) (rural hospitals) via Public Citizen (at-risk hospital designations); Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill (acute-care hospitals); ESRI (one-hour travelsheds); Natural Earth Data (roads, highways, terrain);
Geoff McGhee/& the West
For companies like AMR, which transports roughly one in three air-ambulance patients in the United States, airlifting critical patients to definitive care — by helicopter or by plane — “keeps our ground ambulances serving that local community,” Henricksen said.
In places like the Eastern Sierra, if one ambulance takes a critical patient to definitive care, the round trip can take several hours. For the next 911 caller, the rescue is no longer down the road. Telemedicine, often proposed as a solution for rural communities, does not reliably fill the gap. “Most of my cardiology patients in Bishop don’t have a smartphone,” an internet connection, and technological savvy, Rowan said.
The state-level picture for rural hospitals
Health care researchers have drawn a troubling picture of conditions for rural hospitals nationwide, describing a rural health care system in “crisis.” While the greatest risks of rural closures are concentrated in the south-central U.S., most western states are also showing economic warning signs at their rural hospitals.
Notes: “Risk of closure is defined as financial losses on patient services during the most recent two years and insufficient financial reserves to allow continued operation unless the hospital receives large grants, local taxes, or other revenues not derived from services to patients.“
The cost is a backlog of undiagnosed disease. A woman in Lone Pine showed a sign of advanced heart failure. She’d had bypass surgery six months before, and no cardiac exam before Rowan checked her and found the marker – a 10 percent ejection fraction. Coverage gaps help push cardiac mortality in rural America to rates about 50 percent higher than in cities, according to Rowan.
The “law of small numbers” in rural healthcare


Carmela Coyle, the president and chief executive of the California Hospital Association, calls the underlying problem the “law of small numbers.” A smaller population has a smaller physician workforce, making it hard to keep doctors on call.
It’s one thing for rural Californians to have fewer restaurants or shopping centers. That’s understood. It’s not understood when it comes to healthcare, Coyle said. Like fire stations or police stations, healthcare “is something we need close by,” she said. “When it’s your loved one and there is an emergency, it can’t be 60 miles away.”
The financial pressure that produces care gaps is intensifying. At the start of 2026, 44 percent of all California hospitals were losing money on each patient seen, according to the California Hospital Association. This pressure falls the hardest on rural hospitals.
The same arithmetic applies to ambulances; Henricksen calls this “the cost of readiness.” In a rural community, while there may be only a handful of 911 calls in a given shift, an ambulance must be staffed, fueled, and ready to roll. “The challenge often becomes how you fund those services when there is not enough revenue reimbursement coming in,” he said. Some California communities passed tax measures to subsidize emergency services; others have not.
The problematic balance sheet

With financial margins thinner, a single decision can tip an entire hospital over. At Northern Inyo Healthcare District in Bishop — the counterpart to Southern Inyo and the only labor and delivery unit for three hours’ drive in either direction, the chief executive officer, Christian Wallis, said the hospital loses roughly $12,000 on every delivery.
“When people are asking why labor and delivery departments are closing all over rural America, it’s because you can’t continue to sustain that loss,” Wallis said. This February, a supplemental state payment he had counted on was abruptly reduced from $9 million to $3 million — a $6 million hole that, Wallis said, put the district in breach of financial covenants with its bondholders.
In far north Humboldt County, Matthew Rees runs Southern Humboldt Health, a nine-bed critical access hospital, more than 50 miles from the next facility. It serves 10,000 residents and operates on about $30 million a year, according to Rees, and this year’s federal reductions cut roughly $1.5 million.
Because critical access hospitals are reimbursed on the basis of their costs, trimming expenses only lowers reimbursements further. California pays just 15 percent of Southern Humboldt Health’s cost to treat the Medi-Cal patients who make up 40 percent of its outpatient business. “The math doesn’t add up,” Rees said. “The cuts get bigger as it goes along.”
Salinas Valley Health System on California’s central coast loses $180 million a year caring for Medicare and Medi-Cal patients, with commercial insurance subsidizing the rest, according to Dr. Allen Radner, the chief executive. Just to the north, Watsonville Community Hospital is “living on fumes,” he said, sending hundreds of patients Radner’s way because it cannot provide the necessary services.
Surviving, or not
Cottage Health, the largest not-for-profit health system on California’s Central Coast, projects that a five percent annual reduction in reimbursement — more than $50 million a year — will phase in the next three to four years. “The pressures are real in our industry right now,” said Scott Wester, Cottage Health’s chief executive. Wages are rising faster than reimbursement rates, and tariff-driven drug prices are outpacing them further.
“This isn’t just a rural hospital problem,” Radner said. “This is a hospital problem.” Roughly half of California’s 400 or so hospitals are in economic distress. The rural ones, Radner said, “may be the first ones to go.”
Some already have.
Madera Community Hospital, in the Central Valley, shut down in 2023. When it reopened in 2025, it was little more than an emergency department; three affiliated rural clinics — Madera Medical Clinic, Chowchilla Medical Clinic, and Oakhurst Medical Clinic — remained closed. This illustrates what Donaldo Hernandez, former President of the California Medical Association, describes as the unraveling of a healthcare continuum. When a hospital fails, he said, doctors leave and the loss “ripples throughout the entire community.”
Madera now intends to apply for some of the new $25 million emergency state grants for at-risk hospitals. A new report by the advocacy group Public Citizen lists 15 hospitals at risk of closure in the Central Valley and two more in the Imperial Valley. Ten in Colorado are in a similar situation; eight more in Idaho.
Losing its rural designation can be fatal for a hospital. Cal Matters reported that Glenn County Medical Center in the western Sierra lost potentially 40 percent of its revenue after federal regulators recalculated its distance from the next hospital as three miles below the required 35-mile distance. New calculations found the next hospital was 32 miles away — though the county argued the route that most ambulances drive is 35.7 miles. The medical center is set to close this fall; 28,000 county residents face at least a 40-minute drive for emergency care.
The patients who get hit the hardest

The map of who gets left behind is determined not only by distance, but also by identity.

Angela Williams, a Stanford undergraduate, grew up in a Bakersfield farmworking family in the Central Valley, which is the agricultural heart of the country. “We’re picking the food for everyone else, but we don’t see any of those benefits,” she said. “It’s at the cost of our own health.”
For Native communities, the strain is compounded by the chronically underfunded Indian Health Service. Williams’s grandmother, elderly and unable to drive, lives near a reservation in Oklahoma with tribal resources she can’t reach. Her father, on Medi-Cal in Bakersfield, refused to call an ambulance after a car accident, afraid of the cost. He toughed the night out alone with a collapsed lung and concussion, and was rushed into the hospital the next day anyway.
AMR’s ambulance service covers much of California; rates vary but run into thousands of dollars. In Santa Barbara County, most of which is rural, supervisors in 2025 approved a contract raising AMR charges 35 percent: $2,993.88 for basic life support transport and a per-mile charge of $89.99. Medicare and Medicaid reimburse medically necessary transport.

Rural regions can also carry a heavy environmental burden, said Dr. Kari Nadeau, chair of the Department of Environmental Health at the Harvard T.H. Chan School of Public Health. Rural populations are more vulnerable to extreme weather: “There’s such fragile infrastructure that it doesn’t allow for a lot of mobility… when there is an extreme weather event associated with climate change.”
People living near forests that burn repeatedly breathe wildfire smoke year after year, Nadeau said; long-term wildfire exposure is linked to higher rates of cancer, respiratory symptoms, and neurological impacts.



Signed in July 2025, the “One Big Beautiful Bill Act” will cut federal Medicaid funding by more than $1 trillion over the next decade, with the heaviest impact beginning in 2027 and 2028. In anticipation, some California hospitals are already laying off workers and closing services. “This could look more like a tsunami wave of service closures,” said Coyle of the California Hospital Association. The Medicaid funding cuts are layered atop the hangover of the COVID-19 pandemic. Then, federal government funding was briefly robust. Until that ended.
When Southern Inyo’s Kevin Flanigan arrived in August, the facility was not just cash-strapped, but on the edge of bankruptcy: eight days of cash in the bank, $4 million in unpaid vendor invoices, and staff who had gone unpaid over the holidays but kept coming in to see patients.
COVID-19, Flanigan said, disguised deeper troubles. “Money was free-flowing, and it masked some operational concerns,” he said. “Those [hospitals] who recognized and fixed it are doing fine. But those who didn’t ended up in crisis, and we were one of those.” Closure is self-defeating, he added, because “it is far less expensive to keep a hospital open and operating than it is to let it close and try to reopen it again.”
Southern Inyo Hospital has engineered a turnaround after negotiating vendor payment schedules and reducing payroll costs. But Flanigan is clear-eyed about the trouble ahead: “We’re staring down the barrel of dramatic federal cuts. Right back where we were.”
In late 2025, the Centers for Medicare & Medicaid Services launched a $50 billion Rural Health Transformation Program, of which California was awarded $233 million to build a rural care model, develop its workforce, and expand technology. But the $50 billion is slightly more than one-third of the $137 billion KFF calculates rural hospitals will lose under the OBBBA. It also comes with restrictions, including limits on using it to pay for services to keep struggling hospitals open. “We need to keep the rural hospitals open first before we can innovate,” Coyle said.
Hernandez calls the program “woefully inadequate” compared to what had been lost: “You took away a meal from a starving person,” he said, “and gave them some peanut butter crackers.”
Harvard’s Nadeau hopes that the $50 billion will “modernize technology and expand the workforce,” by building decentralized healthcare infrastructures that can stand on their own.
What next for rural hospitals?

Many rural hospitals are improvising. One strategy is to stop competing and start collaborating. In Lone Pine, rather than each facility chasing its grant money alone, Wallis’s group is bundling into a single application: three hospitals — Northern Inyo, Southern Inyo, and Mammoth — plus the Toiyabe tribal health clinic, spanning two counties and anchored to a larger trauma center in Reno that can take the most serious cases.
“Normally, we all operate in silos,” Wallis said. “But if we can create this rural clinically integrated network, that’s what the transformation dollars were meant for.”
This Eastern Sierra coalition is not inventing its model from scratch. In North Dakota, 22 independent rural hospitals have banded together as the Rough Rider Network. Serving 225,000 people combined, these hospitals are negotiating for better prices on everything from mobile MRI units to value-based contracts — all without selling out to a larger system.
In Colorado and eastern Utah, a coalition of rural hospitals, the Community Care Alliance, plans a joint venture with the Eastern Plains Health Consortium. The goal: improve care coordination and give the new network, with more than 40 hospitals or primary care providers, a better bargaining position, Becker’s Hospital Review reported.
In Montana, Modern Healthcare reported that 24 critical access hospitals launched the Yellowstone High Value network in May 2025 to coordinate care and negotiate contracts on a scale that none could reach alone. This allowed independent rural hospitals to act to their fullest capacity without selling out to a larger system. Similar alliances have taken shape across the West, from Nevada to the Mountain West and western plains to Oregon.
Rethinking the rural workforce
On the workforce side, Coyle’s prescription: use personnel strategically, so “everybody is practicing at the top of their license,” leaning on nurse-midwives, doulas, and community health workers alongside physicians. “When we have limited healthcare professionals, we need to be using every hour of their time as efficiently and effectively as we can.”
But the workforce problem is worsening: across the Mountain West, Utah has roughly 1.4 nurses per 100 people, the lowest ratio in the country, while Idaho, Wyoming, Arizona, and Colorado are all at least 25 percent below the national average.
Healthcare access, from the perspective of ambulance caregivers, including emergency medical technicians (EMTs) and paramedics, “looks fundamentally different today than it did 30 years ago,” Henricksen said. In rural communities, AMR has developed a Nurse Navigation program to triage 911 calls, connecting less-urgent complaints to primary care or telehealth, without dispatching an ambulance.
Flanigan, the Southern Inyo CEO, is oddly still hopeful. “I find a lot of excitement in what the future holds, by virtue of the fact that no one has any idea what it holds,” he said. “It’s a blank canvas. We’re at an inflection point where people are willing to consider that we have to do a completely different system if we’re going to have these rural areas survive.”
However the healthcare system transforms in the rural West, the need will not relent. “People aren’t going to be any less sick,” Coyle said. “There won’t be fewer accidents, fewer cases of cancer, and all the rest.” Recently, Coyle heard a line she has not been able to shake: “Where you choose to live should not determine if you live or die.”
In the Eastern Sierra, that’s no longer just a slogan.
Edited by Felicity Barringer.

For rural western hospitals, “distance is the emergency” – but not the only one
Already faced with extreme distances and a low population base, rural hospitals are being put on their heels by federal funding cutbacks. Specialty care is increasingly difficult to supply and closures loom as a possibility for dozens of facilities.

Buried in the soil or drifting on the wind, Valley fever fungus spreads further around the Southwest
“The West’s Lyme disease” gets less attention as cases rise – even while drastically undercounted. Climate change and land development are worsening the picture.

Paradise’s recovery from the Camp Fire became harder when the only hospital left
Years after a devastating fire, a recovering city finds itself a health care desert.

Urban, rural and tribal: how three Wests diverge on cannabis
The West led the charge to legalize marijuana. As it becomes big business in many cities and towns, some others view it with distaste grounded in moral qualms or concerns about criminal cartels. Will growing revenues help sweeten the pot?

To Fight a Plague, Local Governments Lean on Trust. Could They Lose It?
To keep the virus under control and health-care resources within capacity, counties and towns rely on trust and try to cajole residents to comply with mandates, rather than punish them for flouting rules.

By Treating Obstacles to Health, Community Health Workers Also Treat a Troubled System
Welcome to the world of community health workers. The job, part medical aide and part social worker, is a tradition in poor and rural communities around New Mexico and well established in similar places around the country. But institutional recognition has been slow to come.